Key Take Outs
Enzyme development
Jump to sectionMotility development
Jump to sectionMicrobiome development
Jump to section
Infant digestive system development
Proper nutrition is crucial in supporting healthy growth and development during the first 1,000 days of life as the digestive system develops.
Illustration of the first 1,000 days
The first 1,000 days of life is a period of rapid growth and development, including a baby’s digestive tract and brain, as they continue to develop outside the womb. During this time, the digestive system is still developing as certain enzymes, the microbiome, and motility mature.
See ‘How nutritional changes can impact digestive comfort and support gut health’ to find out more.
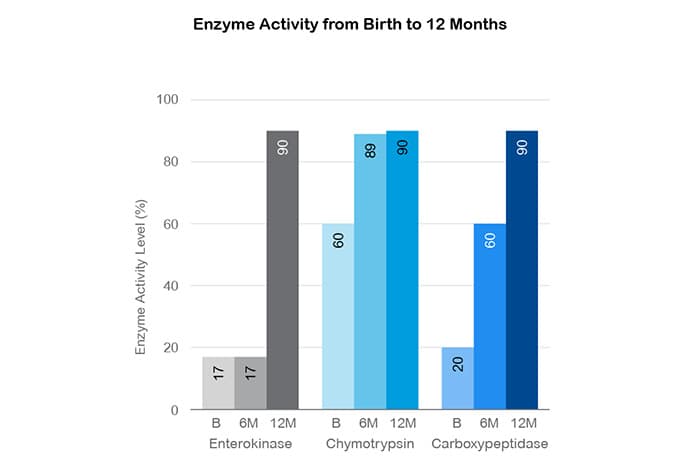
Enzyme development
Decreased activity of protein enzymes can result in difficulty to digest proteins.1,2 For example, protein enzymes like enterokinase, chymotrypsin, and carboxypeptidase do not reach maturity until 2 years of age.3,4 Similarly, lactase enzyme activity can be lower at birth, which can reduce the ability to break down lactose.5,6
During this time, the digestive system is still developing as certain enzymes, the microbiome, and motility mature.
Motility development
Motility of the GI tract, or peristalsis, also continues to mature during the first year of life.7 Additionally, the lower esophageal sphincter, which controls the flow of food from the esophagus to the stomach, does not function in a mature way during infancy and can allow stomach contents to flow back into the esophagus.8,9
Microbiome development
The gut microbiome, which consists of microorganisms that live in the digestive tract, also plays a significant role in digestion and nutrient absorption.10 Although the colonization of these microorganisms starts in the womb, the microbial makeup gradually shifts and reaches adult-like composition around 3 years of age.10
- Berseth CL: Probiotics in the prevention of necrotizing enterocolitis in preterm infants: A multicenter, randomized, controlled trial. Clin Pediatr (Phila) 2009, 48(1):58-65.
- Neal-Kluever A, Pavlidis P, Matthews T, et al.: Drug metabolism and disposition in pediatric populations. Drug Metab Dispos 2019, 47(3):296-313.
- McClean P, Waver LT: Pediatric gastrointestinal problems: A review of clinical issues. Arch Dis Child 1993, 68(1 Spec No):62-65.
- Cuadros-Mendoza CA, Barrera C, Palacios-Moreno D, González-Monroy M: Prevalence of functional gastrointestinal disorders in Mexican children. Acta Pediatr Mex 2017, 38(3):182-201.
- Romero-Velarde E, López-Teros V, Hernández-Bonilla D, et al.: The effect of dietary interventions on pediatric gastrointestinal disorders. Nutrients 2019, 11(11):2737.
- Fawley R, Heitlinger L: Lactose Intolerance in Children. American College of Gastroenterology website [Internet; updated 2021; cited 2024 Aug 29]. Available from: https://gi.org/topics/lactose-intolerance-in-children/
- Jadcherla SR, Berseth CL: Gastrointestinal disorders in neonates: Nutritional strategies and management. In: Neu J (Ed.), Gastroenterology and Nutrition: Neonatology Questions and Controversies. Elsevier Inc.; 2012:27-37.
- Stanford Medicine Children's Health: GERD (Gastroesophageal Reflux Disease) in Children [Internet; cited 2024 Aug 7]. Available from: https://www.stanfordchildrens.org/en/topic/default?id=gastroesophageal-reflux-disease-gerdheartburn-in-children-90-P01994
- Yale Medicine: Pediatric Reflux Disease [Internet; cited 2024 Aug 29]. Available from: https://www.yalemedicine.org/conditions/pediatric-reflux-disease#:~:text=The%20muscle%20in%20their%20lower,they%20are%202%20years%20old.
- Yang I, Rhee C, Wu M: The role of nutritional interventions in pediatric reflux disease. Nurs Res 2016, 65(1):76-88.


.webp?width=1200&quality=75&auto=webp)